Are You Injury Prone? How Genetics Relate to Chronic Injury (and What to Do About It)

by Scott Hogan, ACE-CPT, COES
If you are injury-prone (like me), you may be wondering if there is a genetic component to getting hurt all the time. Or, if you should blame it on nutrient deficiencies, being clumsy, or simply bad luck.
Depending on your frame of reference, the phrase injury-prone might project images into your mind of an awkward kid stumbling along with his shoelaces untied. If you’re an athlete or fan, you might envision your favorite NFL quarterback who simply cannot stay off the injured reserve list.
I have a more personal relationship with being injury-prone. From the time I was a little kid, I suffered injuries that sounded made up to a 10-year-old. I still remember when our family physician told me that the chronic pain in my heels was from something called plantar fasciitis.
Later, after suffering an elbow injury from throwing a baseball, the doctor told me I had something called Little Leaguer’s Elbow (“c’mon Doc, you just made that up,” I thought).
Fast-forward a couple of decades, and I’ve made a career out of getting hurt, finding ways to fix it, then helping other people do the same. When I first started my research into the science of being injury-prone, I had a hunch there was more to it than bad luck or not drinking enough milk.
It turns out that what we see in news headlines or fitness articles is only the tip of the iceberg. The science of being injury-prone is almost endlessly complex and fascinating.
This article aims not to cover every possible variable, but to provide a broad sweeping picture of the injury-prone landscape, highlighting the most impactful variables. And of course, to give you actionable intel on how to be less injury-prone.

Injury-prone definition and risk factors
The dictionary definition of injury-prone is being “frequently injured.” However, only measuring the frequency of injury does not give us a full picture of variations that make some people more likely to become injured than others.
Among the endless list of factors are genetic traits, anatomical makeup, gender, disease states, exercise and lifestyle habits, nutrient deficiencies, environment, risk-taking, and of course, history of injury.
To understand what injury-prone really means, we need to understand what the most common and impactful variables are that lead to frequent strains, sprains, breaks and tweaks.
🔬 How to tell if you are injury-prone
If you answered yes to most of these questions, you can safely assume that you are more injury-prone than the average person:
- Did you suffer more injuries as a child than your friends and peers?
- Do you have two or more body parts (e.g. joints) that suffer recurring injuries and pain?
- Do you have a family history of common injuries? (e.g. you and your father suffered Achilles tendon injuries)
- Do you suffer daily from joint pain and aches?
- Do activities that other people do without injury often cause you pain and injury?
Acknowledging that you are injury-prone is not an admission of weakness, nor is it an excuse to stay away from activities you want to pursue. It’s simply a factor you should consider to help you stay healthy and pain-free as you move your body through life.
Soft tissue overuse injuries as a key driver of being injury-prone
In high-contact sports such as football, soft tissue injuries (muscle, tendon, ligaments, etc.) account for about 70% of visits to physical therapists.105 Most of those involve connective tissue rather than just muscle, with at least half coming from overuse injuries rather than sudden acute injuries.
According to the Centers for Disease Control (CDC), these figures roughly apply to youth and weekend-warrior adults as well as serious athletes:
- Overuse injuries account for about half of all sports injuries in middle school and high school aged students.
- Since 2000, there has been a fivefold increase in shoulder and elbow injuries among youth baseball and softball players.
- The parts of the body most frequently injured while engaging in sports and recreation activities are the lower extremity (42.0%), upper extremity (30.3%), and head and neck (16.4%).
- More than half of all sports injuries are preventable.
From this data and my experience, it’s clear that (a) soft tissue injuries should be the main point of focus for preventable injuries and mitigating injury risk, and (b) overuse injuries are the primary driver of being injury-prone in both athletes and non-athletes.
🔬 What is the most injury-prone sport?
Despite perceptions of football and soccer causing more injuries, statistics show that basketball is the most injury-prone sport. Beyond ankle sprains and knee injuries, basketball players often suffer broken bones, injuries to the face, and other contact-related injuries.
Factors that determine being injury-prone
If you’ve ever wondered if there is a genetic component to being injury-prone, the answer is yes. Beyond the obvious variances in anatomy, there are specific gene variations that have been linked to increased injury risk:
Genetics and disease-related factors for being injury-prone
If you’ve ever wondered if there is a genetic component to being injury-prone, the answer is yes. Beyond the obvious variances in anatomy, there are specific gene variations that have been linked to increased injury risk.
For example, the COL1A1 gene has been linked to decreased risk of soft tissue ruptures, such as Achilles’ tendon and anterior cruciate ligament (ACL) injuries. Researchers believe this rare genotype has a protective effect against injuries. Genetic testing in sports to help predict and prevent injuries is now a big business.
Both heritable diseases and diseases of lifestyle are also significant causes of injury-proneness. There is a whole cluster of disorders referred to as type II collagenopathies in which collagen is abnormally formed in cartilage structures.
Other common diseases that affect injury risk include Ehlers-Danlos, gout (gouty arthritis), fibromyalgia, and hypothyroidism. The ways in which these diseases cause injuries vary widely. For example, hypothyroidism causes a buildup of glycosaminoglycans in the extracellular matrix of tendons, which could predispose the tendons to develop calcific deposits. This is why tendinitis is common in patients with hypothyroidism.
Gout, when there is too much uric acid in the blood, can also cause joint pain and injuries. Uric acid crystals form in joints, causing swelling, pain, and movement dysfunction. People diagnosed with Ehlers-Danlos syndrome often suffer injuries due to hypermobility, including muscle strains, spine deformations, and joint dislocations.
Disease states that affect healing or soft tissue composition can lead to increased injury risk. Even if you haven’t been diagnosed with one of these diseases, it is helpful to realize there are wide variations in how our bodies form tissue structures and respond to environmental stressors.
Physiological and anatomical factors for being injury-prone
Understanding how your anatomy makes you more likely to suffer from certain injuries is a valuable prevention tool. This should inform how you exercise and what movements to be cautious of. Covering all anatomical variations is beyond the scope of this article, so we will dive into a few of the most common physiological variables.
At a basic level, your body type is one of the most important factors to understand for preventing injury. The three body types, or somatotypes, are ectomorph, mesomorph, and endomorph.
Ectomorphs are tall and lean, with small joints, low body fat, and difficulty maintaining muscle mass. Endomorphs are on the opposite end of the spectrum. They have higher body fat levels, gain weight more easily, and have thicker bones and joints. Mesomorphs fall somewhere between these two. They are the most athletically inclined, with high muscle mass and low body fat levels, and solid, proportional joint structures (picture the square-jawed, superman body type).
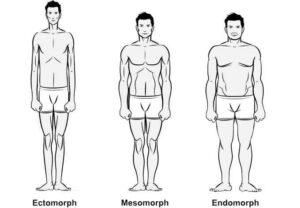
The three somatotypes: ectomorph, mesomorph, and endomorph
Because ectomorphs have smaller joints with less muscle to support them, they are more susceptible to overuse injuries. Exercises that not only build muscle mass but also improve tissue resiliency through full ranges of motion are especially helpful for preventing injury in this body type.
In high contact sports like rugby, endomorphs with a higher BMI (body mass index) are more likely to suffer injuries. This is likely caused by a combination of the nature of their role in competition, powerful muscles, and more limited ranges of motion. Extra body weight also exposes endomorphs to increased chances of injuring their hips, knees, and ankles.
Within these body type differences, there are more subtle anatomical variations that affect injury risk. Here are some common examples:
- Tendon insertion points: There are wide variations among people in tendon insertion points (called the myotendinous junction). A tendon insertion point close to the joint means a relatively longer muscle and shorter tendon attachment—a tendon insertion point far from the joint means a longer tendon and shorter muscle body. You can see this difference most visibly in calf muscle anatomy variations among athletes. As you might expect, a longer tendon insertion increases relative stress on tendon structures during movement.
- Thickness of bone shafts and joints: Athletes with more bone and joint mass are more protected against bone breaks, joint dislocations, and sprains.
- Flat feet: While some people do not experience any symptoms, flat feet put you at risk of more frequent knee pain and advanced knee cartilage degeneration.
- Ulnar impaction and wrist injuries: Ulnar impaction syndrome is a degenerative wrist condition caused by excessive loading stress from abnormal cartilage structures.
- Bone spurs: Some people are genetically prone to growing bone spurs (also called osteophytes), which can rub and fray connective tissue.
- Limb length: Longer limbs create opportunities for ranges of motion that go beyond what joints can safely handle. For example, long-limbed athletes will be more likely to injure their shoulders during a bench press if they bring the bar down to chest level.
- Healing capabilities: There are wide genetic variations in both inflammatory responses to injury and how effectively the body creates, synthesizes, and rebuilds collagen structures. This is a crucial factor not only for being injury-prone, but also for how fast you can safely return to activity.
[See Related: The Definitive Guide to Collagen Synthesis: What It Is, Why It Matters, and How to Increase It Naturally]
Exercise and lifestyle variables that affect injury-prone status
Beyond genetic and anatomical factors that can make you more or less injury-prone, there are several lifestyle factors that come into play. Unlike many diseases or your natural physiology, these are variables you have control over. The most important are your personal injury history, movement habits, and exercise programming considerations.
- Movement habits: People with a sedentary lifestyle who are unaccustomed to physical exertion and activities that require strength, coordination, and mobility are more at risk of suffering injuries when performing activities that require those skills. Beyond movement volume, movement variety is also a leading indicator of being injury-prone. The narrower your movement habits, the more injury-prone you are. Participating in various forms of exercise, active hobbies, and novel movement patterns is one of the best ways to ward off injury.
- Injury history: Any time you suffer an injury, be it a muscle tear or joint sprain, a process of self-perpetuating tissue damage, inflammatory responses, and altered movement mechanics is set in motion. This is called the cumulative injury cycle. It explains why injuries are likely to reoccur, even if you feel as if you fully recovered. It also explains why injuries in one body part can lead to injury and dysfunction in another. For example, hip pain and dysfunction increase your knee injury risk. Further, injuries to connective tissue (namely, tendinopathy) are characterized by parts of the tendon effectively dying off. Again, while you can fully recover and experience no pain, there will always be a risk of recurring pain and injury in the same joint.
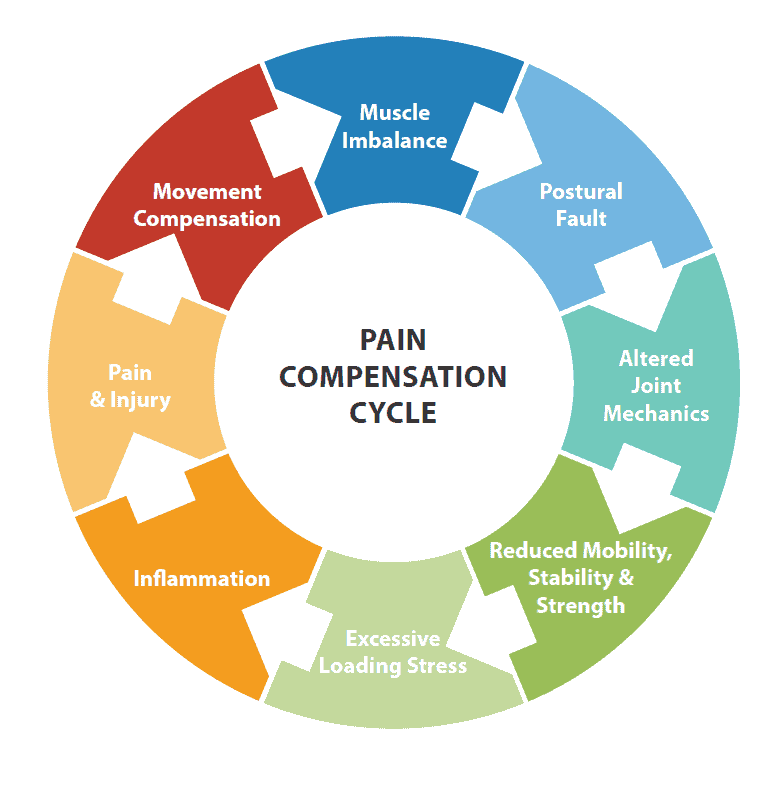
A history of injury can lead to muscle imbalances and movement compensations that predispose you to future injuries.
- Muscular imbalances and poor exercise habits: Lopsided exercise routines can cause muscle imbalances that predispose you to injury. One of the most common examples is the tendency for people to overtrain pushing movement (e.g. bench press), while neglecting pulling movements (e.g. rowing). This creates tight chest and anterior shoulder muscles and weak, stretched-out upper back and posterior shoulder muscles. While the term muscle imbalance is often used to describe muscle asymmetries that affect aesthetics, the most important consideration is how muscle imbalances create unnatural movement patterns and loading stress that can lead to injury.
- Inadequate exercise programming: The most important principle to get right when constructing your exercise plan is to prevent accumulated joint stress. Because tendons and ligaments heal more slowly than muscles, you must balance muscle and strength gains with joint recovery. Along with utilizing rest days and low-intensity training days, and adding more movement variety, scheduling a deload week every four to eight weeks will go a long way toward letting your joints repair. Deload simply means backing off the intensity and/or volume to allow muscles, the central nervous system, and connective tissues to heal optimally. Another important consideration is matching training demands to those faced during events or competitions. Tim Gabbett, one of the world’s leading injury prevention experts, describes a phenomenon called the injury prevention paradox, which states that high-volume training has a protective effect against injury. And that while overtraining is a common cause of injury, undertraining that does not prepare athletes for the demands of competition is just as common.
🔬 The danger of isolation: how exercise selection can make you more injury-prone
Overdependence on isolation exercises (e.g. bicep curls) and repetitive movements make you more injury-prone in three distinct ways:
- Exercises that isolate only one or two body parts build muscle strength in a small area while neglecting adjacent muscles. The gap between strong areas and weak areas is where injuries occur.
- Limited movement variation creates strength and coordination through limited ranges of motion. If you’re strong through the top 80% of a joint’s range of motion (ROM) but have virtually no training through the bottom 20%, your injury risk is increased.
- Isolation movements by definition target only the prime mover muscles—the ones that directly cause the desired motion. This leaves out the supporting cast of stabilizer muscles that are necessary for safe, functional movement in the real world.
While isolation exercises can be part of a successful training program, the majority of your training should involve compound movements that challenge multiple muscle groups and joint systems together.
- Nutrient deficiencies: Deficiencies of energy (calories), vitamins, minerals, and protein impair injury healing and speed up the loss of muscle and connective tissue mass after exposure to physical trauma. This principle does not just apply to post-injury care, but also daily nutrition habits that allow your muscles, joints, and bones to recover from the stress of training and lifestyle demands. Calcium, magnesium, vitamin D, and iron are some of the most common nutrient deficiencies that can make you more injury-prone.
- Bodyweight: Though bodyweight certainly has a genetic component, lifestyle behaviors that lead to increased overall body weight (i.e. poor exercise and nutrition habits) increase injury risk, especially in the knees and lower extremities.
- Risk taking: Though the research is ambiguous, risk-taking is a common sense factor for being more or less injury-prone.
- Environmental factors: Where you live affects your injury risk. Environmental factors such as temperature, humidity, and even oxygen levels all play a part. For example, cold weather reduces tissue temperatures, blood circulation, and nutrient delivery to working muscles and joints. This causes increased metabolic demands and reduced stamina, which both make you more injury-prone. From a preventive standpoint, preparing your body with incremental environmental exposure is an effective injury prevention strategy.
Are women athletes more injury-prone than men?
A common question I get is “are women more injury-prone than men?” For most overuse and repetitive use injuries, the answer is yes. There are a few specific injury types that female athletes should be aware of to help prevent problems before they occur. Women are more likely than men to suffer common lower body sports injuries, like ankle sprains and knee ligament tears, because of differences in anatomical build and hormonal variations.
In fact, studies show that female athletes are three times more likely to suffer an anterior cruciate ligament (ACL) injury than male athletes. Researchers believe this is caused by a smaller ligament cross-sectional area and a more narrow intercondylar notch within the knee joint.
Muscle imbalances are also at play. Women are more likely to have extension-flexion imbalances in their leg muscles (i.e. stronger quadriceps compared to their hamstrings). This imbalance causes a movement fault called knee valgus, where the knee caves inward during landing and jumping.
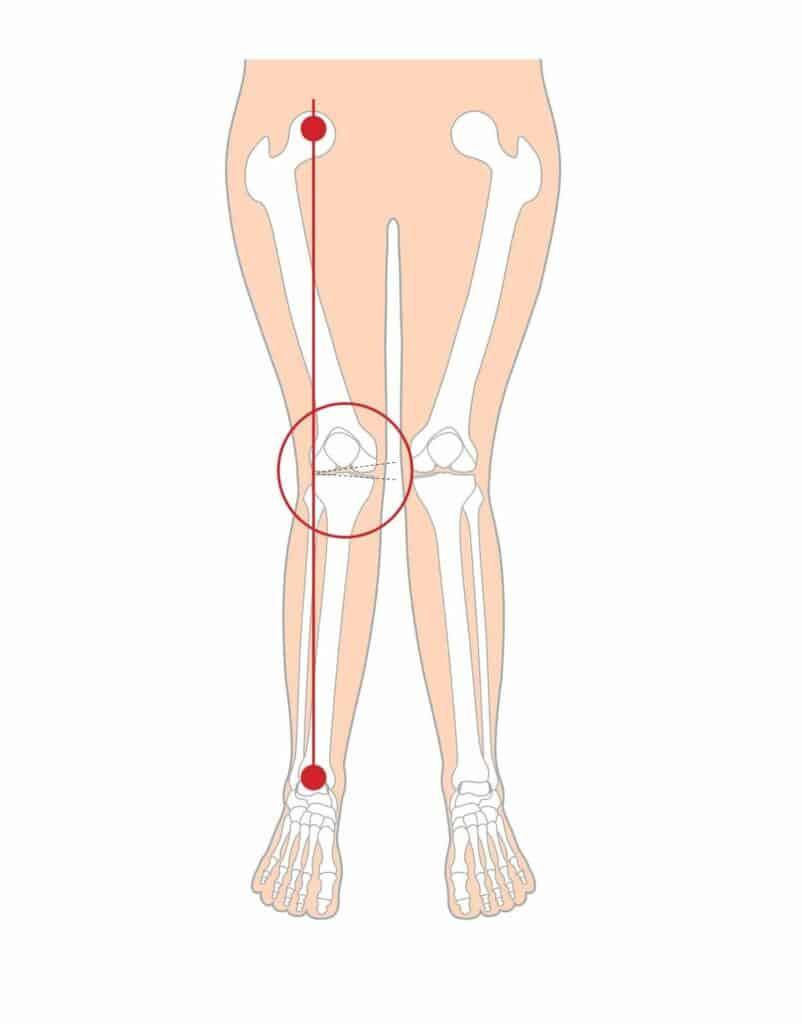
Illustration of a knee valgus movement fault
Women also have higher estrogen levels, which reduce tendon stiffness and ligament strength. Especially immediately post-puberty, when estrogen levels spike, female athletes are at a greater risk of developing tendinopathy or suffering a tendon rupture. More joint flexibility and cartilage laxity also put female athletes at a greater risk of suffering shoulder, hip, knee, and ankle injuries.
Finally, there are a few common nutrient deficiencies in women that increase injury risk, namely protein, calcium, iron, and vitamin D. These nutrients are essential for connective tissue healing and bone mass maintenance.
Male athletes have their own specific risk points. Men are more likely to suffer from acute injuries than women. Anatomical differences can favor women as well, with men suffering from certain hip and groin injuries, especially from tight muscles and joints, more often than women.
Understanding these risk points can help female athletes prevent injuries. For example, increasing hamstring exercise volume, perfecting landing form to avoid knee valgus, and resistance training with slow, deliberate repetitions are all strategies women can implement to counteract injury risk.
What you can do to mitigate injury risk
As counterintuitive as it sounds, the best way to mitigate injury is by understanding what to do when you become injured and after you become injured. As in many other arenas, history is the best predictor of the future. So it follows that beyond taking basic preventative measures, having a solid understanding of post-injury care and rehabilitative concepts will armor you against future problems.
What to do before you get hurt (prevention)
An ounce of prevention is worth a pound of cure. Nowhere is this truer than in injury management. Understanding your genetic and anatomical risk factors, constructing an exercise program that prevents joint stress accumulative and muscle imbalances, and avoiding nutrient deficiencies will all help you avoid injury.
But the best injury prevention technique is behavioral and much more subtle. Virtually every injury I have experienced or coached an athlete through was preceded by pain sensations, altered joint mechanics, or some movement variation. Sensing these precursors to injury and acting accordingly is the ultimate injury prevention hack.
What to do when you get hurt (mitigation & understanding)
Think about these questions after an injury to make sure you understand and address the underlying causes (instead of merely addressing symptoms):
- Is it an acute injury (from a traumatic event) or overuse injury (symptoms increased gradually over time)? Could it be a combination of the two?
- Were you experiencing any ongoing pain, tightness, or discomfort in the weeks leading up to the injury? If so, that indicates a chronic injury and connective tissue degeneration that will need to be rebuilt.
- Are there movement patterns involving the injured body part that you were not able to correctly perform before the injury? This indicates a movement fault that led to repetitive tissue stress.
- Do you have a history of injury at or around the injury site? If so, that indicates you may have scar tissue buildup and mobility deficits that make you prone to future injuries.
- Can you think ofany repetitive motions involving the injured body part that you performed regularly leading up to the injury? If so, seek to understand what kind of muscle imbalances that repetitive motion creates, what tissues it could degenerate, and what you can do to reverse the effects of the repetitive motion. Finally, find ways to reduce chronic stress from repetitive motions in the future.
- What postural faults do you have that deviate from optimal static posture? This gives you insight into which muscle imbalances you are at risk of developing that could lead to injury.
What to do after you get hurt (recovery)
Understanding the cause of your injury and developing a rehabilitation plan are the two fundamental steps of injury recovery. The most overlooked aspect of post-injury care is following through with a complete rehabilitation plan. Athletes will commonly start feeling better a few weeks into caring for a minor joint sprain or muscle strain, then cease doing the recovery work responsible for the progress.
A good rule of thumb is to continue any rehabilitative efforts for at least six weeks after your symptoms have resolved. It can take months, or longer, for soft tissues to fully heal and become strong and pliable enough to avoid re-injury.
Injury-prone? You'll love my best-selling corrective exercise book, Built from Broken.
Conclusion
People tend to avoid addressing the underlying factors that make them injury-prone. It’s as if they believe that admitting they have genetic, anatomical, or lifestyle characteristics that make them injury-prone is an admission of weakness. But this is not a smart strategy for avoiding injury.
On the opposite end of the spectrum, becoming overly fearful of injury is not an ideal way to move through life. A helpful exercise is to view your history and anatomy as if you were coaching someone else.
What advice would you give that person?
What topics referenced in this article deserve the most attention?
This can help you build a more objective perspective and strategy. Remember that any variable that makes you more injury-prone is not an excuse, but a factor that should be considered.